Prinz is a 9-year-old German Shepherd mix referred to BVNS for an inability to walk in the hind legs and severe back pain of less than 24 hours duration. The prior afternoon, Prinz had been playing ball. He jumped to catch the ball, and upon landing, cried out, and was immediately paralyzed in the back legs. Over the next 15 minutes, he regained movement in the back legs but was unable to walk. He continued to be extremely painful, even biting his owner when they tried to help him, very atypical behavior for him as he’s normally a lover and very playful. He was rushed to an animal emergency hospital and treated supportively with anti-pain medications, NSAIDs, and fluids.
is a 9-year-old German Shepherd mix referred to BVNS for an inability to walk in the hind legs and severe back pain of less than 24 hours duration. The prior afternoon, Prinz had been playing ball. He jumped to catch the ball, and upon landing, cried out, and was immediately paralyzed in the back legs. Over the next 15 minutes, he regained movement in the back legs but was unable to walk. He continued to be extremely painful, even biting his owner when they tried to help him, very atypical behavior for him as he’s normally a lover and very playful. He was rushed to an animal emergency hospital and treated supportively with anti-pain medications, NSAIDs, and fluids.
Presenting Complaint:
- Peracute paraplegia (loss of conscious movement in the pelvic limbs) and severe back pain after a jump while playing ball.
- Slightly improved neurologic grade, non-ambulatory paraparesis (conscious movement present in the pelvic limbs but unable to walk) and continued intense pain despite analgesics (anti pain medications).
Assessment (Neurolocalization):
Severe non-ambulatory paraparesis, absent postural and placing responses in the pelvic limbs, brisk spinal reflexes with intact superficial pain perception, cutaneous trunci reflex present cranial to T12 on the left and present cranial to L1 on the right, left sided muscle spasms and discomfort extending from T12 to L4/L5.
Prinz’s deficits localized to a left lateralizing T3-L3 myelopathy with the primary differentials being a Type I or Type III disc extrusion.
Diagnostics:
 Spinal radiographs taken by the emergency hospital revealed predominant finding of a subtle narrowing of the T12-T13 intervertebral disc space.
Spinal radiographs taken by the emergency hospital revealed predominant finding of a subtle narrowing of the T12-T13 intervertebral disc space.
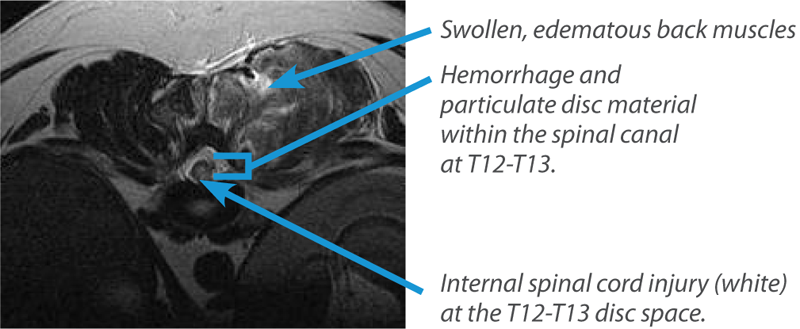
An MRI of the thoracic to sacral spine was performed. Extra-dural hemorrhagic material was dispersed along the left canal extending from T11 to T13 causing mild cord deviation towards the right of the canal. Nearly 75% of the spinal cord parenchyma, slightly left lateralizing but predominantly central in distribution, demonstrated increased T2W signal consistent with edema, dorsal to the T12-T13 disc space. The left paraspinal muscles extending from T9 to L2 were diffusely swollen and edematous.
These findings were most consistent with a high velocity, low volume disc extrusion at T12-T13 and likely concurrent neurogenic myositis or vasospasm with infarction to the left paraspinal musculature.
Treatment:
A left hemilaminectomy was performed from T11 to T13. Upon fascial incision, the left paraspinal muscles everted out the incision margins and were grossly swollen, edematous, and pale. Biopsies were obtained of the abnormal musculature. Upon entry into the canal, the epidural adipose tissue was discolored and intermixed with hemorrhagic material. Tannish fluid like material was removed from the ventral canal dorsal to the T12-T13 disc space. Samples of each were also submitted for histopathological evaluation. Cultures were also collected and submitted. The venous sinus structures lining the floor of the canal were dilated and pulsating. Histopathology results demonstrated myofiber necrosis with neutrophilic inflammation and mineralized cartilage removed from the spinal canal samples. Cultures were negative for bacterial growth.
Diagnosis:
Hansen Type III disc extrusion (high velocity, low volume) at T12-T13 causing internal cord injury and secondary inflammatory muscle necrosis.
Outcome:
Prinz recovered to his normal, active, happy self over the following days and was discharged several days later so he could travel with his family to California where they had recently been stationed. We continue to receive updates from the owner’s regarding Prinz and his life as a “beach dog”! We remain humbled by Prinz’s endearing zest for life and for his military family serving our country.
Take Home Points:
Review of the three primary classifications of Intervertebral Disc Disease:
- Hansen Type I: an acute extrusion, under varying velocities, of the nucleus pulposus (inner portion of the disc, normally gelatinous but can become rock like when degeneration occurs) causing moderate to severe cord compression. Often requires surgical intervention to remove compressive elements and continued cord injury. If the disc material ruptures under high velocity forces,internal cord injury occurs. Less than 1% of patients will develop life ending myelomalacia up to 5-7 days following the injury, despite emergent surgical decompression. MRI often helps identify significant intraparenchymal cord injury and can better help predict prognosis following surgical decompression.
- Hansen Type II: a slow, chronic protrusion or prolapse of the dorsal annulus (ligamentous structure surrounding the nucleus pulposus) into the spinal canal causing slow compression of the spinal cord. One caveat is an “acute on chronic disc” presentation where acute decompensation can occur. If the spinal cord impacts/strikes a mound of protruding dorsal annulus, severe internal cord injury can occur resulting in rapid decompensation.
- Hansen Type III: a high velocity or “explosive”, low volume disc extrusion causing severe internal cord injury. Also referred to as acute non-compressive nucleus pulposus extrusion or ANNPE. If severe enough, myelomalacia, a potentially fatal break down process of the spinal cord, can occur up to 5-7 days from the injury.
To ask a question related to this case or discuss any aspect of it please email Dr. Jarboe.
Case referred to BVNS by Dr. Roque Pereira at the Animal Emergency Clinic of Fredericksburg, Prinz’s primary care veterinarian is Dr. Gary Dunn at White Oak Animal Hospital.
If you would like to download a PDF of the case study, please click here.
-->